Are you helping or just distracting the CNS?
The human nervous system is a very adaptable place. It is constantly reacting to variable stimulus acting on it/us, simplistically we could describe it as input-process-output system although we have to remember processing is often based around a predictive, or more fancily put a Bayesian inference model.
What this means is that if we alter the input we may get a different output in response.
I have read recently much discussion about the CNS being easy to fool and also how we can ‘hack the nervous system’ and in all honesty I am not sure I agree, the CNS is not a computer after all and this to me feels like we imply that, instead I think we probably change the opinion of the nervous system by providing a different temporary input that potentially temporarily alters the outputs. We don’t swap one ‘program’ for another or hit ‘reset’ and go back to factory settings (whatever that may be?) instead the ‘program’ is in a constantly evolving state dependent on the inputs applied. Sure sometimes we get locked in a consistent input-output ‘loop’ but this habit is not often altered permanently instantaneously.
If my output, lets say joint stiffness, is based around the protection of a tissue and I am provided with a bunch of non threatening inputs then my CNS opinion may change to one of ‘we do not need so much protection’ and decrease the output of muscular tension that in turn decreases the joints stiffness. Like most habits the more ingrained it is then the more regularly a ‘positive’ input may have to be applied to change the opinion over the long term.
Is it just distraction?
In some cases this maybe more of a distraction rather than a change in opinion, the novelty and magnitude of an input applied may be far more interesting or noteworthy than the current situation. If I distract the CNS’s attention by providing another more interesting or attention grabbing stimulus then this change in input may alter the CNS output. A distraction may not provide a stimulus to positively change anything long term however.
We can consistently provide distractions without ever fostering an environment for change. How many ‘short-term therapies’ do just that?
This change in output can often be confused with more than just a temporal distraction and this maybe where we start to extrapolate a touch. Suddenly a new input can be the ‘fix’ to a long standing problem in a far away part of the body and any short term change mistaken for a miraculous missing piece to someone’s complex pain puzzle.
We can make up some fabulous back stories to accompany them encompassing the fascial system, biomechanics and fancy brain based mechanisms. All of these ‘fixes’ rely on short-term changes in range of movement, strength or sensation as a marker of success, things that are all also regulated via CNS output! Change does not imply the change is a good one, merely change, short-term change also does not imply a long-term change or ‘fix’.
We can confuse increases in strength of muscles and ROM at joints as a positive. In back pain sufferers an increase of contraction of the core muscles is associated with ongoing pain states, decreased stiffness and muscle length regulation could actually also be detrimental to controlling movement. Both strength and flexibility are context dependant.
An increase in muscle strength in an area of pain is an outcome variable potentially surrogated for the actual problem and more than likely completely unrelated to a cause.
Lets put this into context.
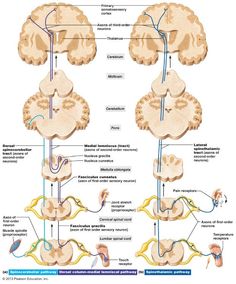
Someone has a pain in the elbow and a therapist or trainer provides a stimulus to the foot. This travels up the various spinal pathways, dependent on the stimulus, to the brain for processing. Suddenly the elbow may feel different better even, does this mean that the body needed a stimulus specifically from the foot and this is linked to the elbow somehow and THE cause of the problem or more simply the CNS has paid more attention to the information coming from the foot, perhaps more compared to other body parts moving, and has therefore changed its output towards other situations it is regulating in the body?
Information burst!
Why would it pay attention to a specific body part more?
Well if we generally have limited movement coming from a joint then the proprioceptive burst of information is going to be new, noteworthy and interesting to the nervous system. We pay attention to stimulus that is new or outside of our predictions that we base on previous experiences. An example would be stepping off a curb that is much higher than normal, we suddenly become aware of this change in incoming information whereas if it were a normal height it would simply not be information worthy of paying attention too and we would walk merrily on unaware. While we are paying attention to this new stimulus the regulation of sensation or stiffness of other areas, especially if the new stimulus is sufficient in duration, might change as they are outputs of the CNS.
It may not be that the two areas are somehow linked and this is THE stimulus someone needs instead it is A stimulus they are paying attention to RIGHT NOW. In fact this level of distraction may change further down the line with the stimulus not creating the same distraction as it now provides less novelty and attention grabbing potential. We see this with soft tissue work, people graduate from foam rollers to harder materials such as kettle bell handles to provide the same level of stimulus that the body/CNS has become used to and no longer has the same effect.
Perhaps the issue that someone had originally has waxed and waned and regression to the mean has worked its magic at the same time and the assumption is the magic was the ‘cure’. This is a great read about why ineffective therapies may appear to work and the real mechanisms that are at play. Why do ineffective treatments seem helpful? A brief review
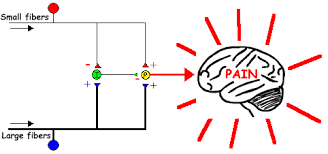
Proprioceptive information created by movement can also have a ‘gating’ effect on pain with large fibre information such as from A beta fibres inhibiting smaller fibre input from A delta and C fibres that carry noxious information. This is why we rub a painful area and is this theory is known as the ‘Gate control theory’ originally proposed by Melzack and Wall. One of the reason this theory has evolved from its original incarnation in 60’s is it requires a nociceptive input for pain, as does another neurophysiological mechanism ‘descending inhibition’, and why the idea of distraction and changing opinion appeals to me more in some cases. The reason I like the idea of a change of opinion or distraction is because it does not imply there is nociception occurring to be inhibited instead just one input competing with another or an input altering outputs.
For someone in pain a distraction may be just what they need, where we run into issues is when the input professes to be more than that with all manner of bizarre back stories, tenuous connections and nocibo inducing blame lumped on various body parts and systems.
Painful therapies or inputs may do something very similar. Foam rolling or a painful sports massage has temporal effects. They make you feel better, or different, but generally in the short term. So let’s say I feel stiff and tight after a hard workout the day before and decide a good foam roll is going to make me feel better. While I am rolling it really hurts, god it hurts, but suddenly I feel a hell of a lot less tight after, could that simply be that that my CNS is paying attention to the NEW painful sensation caused by the foam roller? It is a greater stimulus newly applied and simply overrides the previous sensation and in response to a different input also changes its sensation output.
This input could also alter muscle extensibility and ROM that is also regulated in part, certainly acute changes, via CNS output. One of the regulators of muscle length is how it feels, you stretch a muscle it feels tight and you stop as that sensation builds. If you have a greater sensation competing for attention or distracting the CNS then the regulatory sensation may simply feel less in comparison or the regulatory output has been altered in response to another competing input.
It could be akin to a child selfishly holding on to a ball until someone offers them the distraction of chocolate. To eat the chocolate they must let go of the ball but they may still be a selfish so and so, their behavior has not been fixed they have been merely distracted.
We do have other mechanisms occurring as well with painful stimulus such as DNIC (diffuse noxious inhibitory control). This is where a strong noxious stimulus causes nociceptive neurons to send impulses to the caudal medulla that triggers an efferent inhibition of nociceptive neurons or more simply put pain inhibiting pain! We would however need nociception to be occurring.
Perception, expectation and inhibition
If I have previously had good results from a certain therapy or input then I might expect good results again. My expectation might drive my CNS to take a positive view or opinion of what is occurring. It maybe that the environment or person I am dealing with induces a positive input and a positive output. You feel comfortable, relaxed and safe making your CNS put a positive spin on events.
It could be just the opposite with a cold horrid waiting room and a nasty doctor or a previous bad experience with a dentist, therapist or trainer that changes my CNS opinion or processing of an event with anxiety rising heightening the attention to or processing of any potentially damaging stimulus.
Pain relies in part on the balance between the amounts of endogenous (internally generated) inhibitory chemicals floating around your nervous system versus the amounts of chemicals involved in facilitating the pain experience rather than just a simple causal relationship.
The periaqueductal grey (PAG) can send inhibitory impulses from the brain stem to the dorsal horn via the ventromedial medulla (RVM) and dorsolateral feniculus. The PAG receives inputs from the hypothalamus, cortical regions and the limbic system so these impulses could potentially be triggered by any of the processes arising from these brain areas associated with actions such as sensation, movement, emotion and many more. Within the RVM there is thought to be ‘off’ cells that exert a descending inhibition and also ‘on’ cells that facilitate nociceptive transmission and this has been implicated in chronic pain states. With nociceptive facilitation and sensitization of peripheral receptors we may achieve encoding of nociceptive signals with what would normally be a non-noxious stimulus. We have chemicals such as endogenous opioids and GABA that have an inhibiting effect on pain and also aspartate, glutamate and NMDA that have a facilitating effect. It is certainly not all about nociception however and we can have inhibition and facilitation of the pain experience within the brain as well and not just during nociceptive transmission.
So the nice therapist comes into the relaxing room and gives you an (potentially bullshit) explanation for why no one has been able to help your pain and confidently reassures you that they have the answer. You feel understood and a glimmer of hope rises. Your brain starts pumping out chemicals that may dampen down your anxiety or may cause inhibition or decreased facilitation of any potential nociceptive signaling. Your chemical balance swings towards the ‘negative’ potential for pain. They apply a painful stimulus or burst of new and novel movement information for you and your brain to deal with and suddenly your painful XXX feels different, better even. It feels looser or stronger perhaps. This is awesome but please don’t confuse this change or distraction with a fix.
Whilst short term success is obviously a positive lets not forget it can often be long term changes in behavior that get the greatest successes.








Leave a Reply
Want to join the discussion?Feel free to contribute!