Core stability – Does it matter? A look at the evidence.
There are many methods and treatments, especially relating to lower back pain, that include a focus on ‘core’ and ‘trunk’ stability and activation for the reduction of pain and increase in performance. In part one we will focus on the impact of a ‘core stability’ approach on chronic low back pain cLBP.
It would seem a common prescription for lower back pain would be a program of ‘core stabilization’ or ‘core strengthening’ both from healthcare professionals and the layperson alike. Its widespread clinical use (Xue-Qiang Wang et al 2012) as well as popular media coverage evidences this.
Whilst there are varying powerful theories on activation patterns, implementation and importance of specific structures, this piece will focus on the actual efficacy of the approach by looking at the research and evidence into clinical outcomes such as pain, disability and fear avoidance beliefs.
The bottom line is this is what people really care about, simply if it gets rid of their pain or not. The efficacy of an approach to reduce pain can only be judged on its ability to do so.
By looking at a number of studies, especially systematic reviews or meta analyses this hopefully takes some of these variations into account between study parameters, methodology and sample size.
With such widespread use for cLBP there has to be something in it, doesn’t there?
A matter of timing
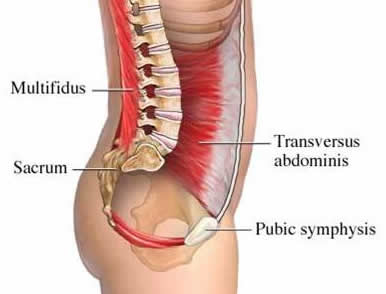
Hodges and Richardson carried out the original research into trunk muscle activation in LBP subjects in the mid & late 1990’s. Much of their focus was on the delay in timing of activation of Transversus abdominis in subjects with LBP. Their conclusion from “Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis” was
“The delayed onset of contraction of transversus abdominis indicates a deficit of motor control and is hypothesized to result in inefficient muscular stabilization of the spine”
They studied TvA and trunk activation in a number of papers including “Delayed postural contraction of transversus abdominis in low back pain associated with movement of the lower limb” and “Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds” with consistent delays in TvA and trunk muscle activation in anticipation of various limb movements recorded.
A lack of lumbar stabilisation was hypothesised to be a factor in pain experience of LBP patients, seemingly with a primary focus on the TvA. This has led to the implementation of exercises to stabilise the lumbar spine and improve the onset of activation of the TvA and other abdominal muscles to reduce ‘instability’ and pain.
One of the first questions we should ask, is the delayed timing a cause or effect of pain? If it is an effect then a focus on the activation may prove to be a fruitless endeavour. That is why we must also look to the research rather than theory as an indicator of efficacy. Are we seeing a correlation rather than causation?
The timing differences that existed between symptomatic and asymptomatic patients were about 20 ms, an exceptionally small measure of time, one fiftieth of a second. The measurements were, it is important to point out, all centred on timing rather than strength, although the terms ‘core strengthening’ has also gained popularity. To my knowledge there has been nothing to suggest increase in strength improves timing. Exercises that focus on conscious or volitional activation may be tough given the that such a small measure of time maybe beyond the conscious control of the patient.
It would also be worthwhile to get a measure of how the muscles of the trunk activate and there relative timings in different movement patterns so as build up a picture of the core's functional performance as well as clinical performance. This may give us a more rounded understanding of the core's activation.
Vasseljen et al (2012) in “Effect of core stability exercises on feed-forward activation of deep abdominal muscles in chronic low back pain: a randomized controlled trial” looked at the change in activation of trunk muscles over an 8 week period in response to a core stability program comprising low load core stability exercises or high load sling exercises. This was as well as a general exercise control group. They then compared feedforward trunk muscle activation to a similar arm movement as performed in Hodges original research.
After 8 weeks of this RCT involving a low load core stability group, a high load sling exercise group and a general exercise group, the onset of abdominal muscles had changed by between 15 and 19 ms only for the high load sling exercises compared to the core stability and general exercise groups.
No actual changes in pain were reported by any of the groups.
They concluded
“Abdominal muscle onset was largely unaffected by 8 weeks of exercises in chronic LBP patients. There was no association between change in onset and LBP”
Moreside et al (2013) also looked at trunk muscle activation in healthy and recovered lower back pain patients in their paper “Temporal patterns of the trunk muscles remain altered in a low back injured population despite subjective reports of recovery”
They found that although the recovered patients, who displayed perceived readiness to return to work and low pain scores, still had an altered muscle activation pattern and greater overall amplitudes of muscle activation.
In these cases it would appear that a restoration of ‘normal’ muscle activation timing and activity was not necessary for their pain experience to subside or caused the pain experience to subside. Equally it proved fruitless to attempt to change these activation patterns significantly with both high load and low load exercises. Any change recorded did not correlate with a reduction in pain.
It maybe suggested that these people were not actually free from the problem as they still displayed muscle activation changes. This cannot be ruled out. A follow up to see if pain and/or muscle activation changed in the future would shed more light on this. However focusing on the timing of activation of the trunk did not seem particularly effective in the cases here in the time frames studied.
In normal day-to-day treatment clinicians do not have expensive EMG machinery to identify apparently ‘faulty’ firing patterns. The only measures that can be used are perceived readiness and pain scores.
Hodges, alongside Tucker, in their 2011 paper “Moving differently in pain” gives a different perspective to the activation of muscles in chronic pain patients.
“Existing theories predict relatively stereotypical change in whole-muscle behavior, but this has not been observed, and variable patterns of adaptation are identified in clinical populations”
He goes on to say
“changes in behavior of other muscles are unique to the individual and possibly to the task. This is most common in complex systems such as the trunk, where the muscle system has considerable redundancy (multiple muscles achieve a similar goal)”
The fact that we see no stereotypical change in muscle behavior should limit our attempt to create a consistent stereotypical behavior. How do we know what to change muscle behavior too? If multiple muscles achieve a similar goal then different people may use different muscular strategies to get the job done. There is a huge possibility that there is no ‘right’ way but many ways between the muscles associated within the task and varying from task to task, activation being function specific.
One of my favourite quotes is from famous British anatomist Charles Beevor in the 19th century. He simply stated in Beevors Axiom:
"The brain does not know muscles only movement"
He also gave a 1903 address to the royal college of physicians entitled "On Muscular Movements and their Representation in the Central Nervous System" This is simply way ahead of its time!
A redistribution of intra and inter muscular activity and mechanical behavior has been proposed to protect against pain and redistribute load. This could also happen when there is also the threat of pain. Inhibition and excitation in painful and surrounding areas/muscles has been clinically documented (Hodges 2011). The outcome goal of the activation pattern/timing would be to provide a protective strategy.
The nervous system may have a huge range of peripheral and central options to increase, decrease or redistribute activity. Such as motor neuron excitability, cortical inhibition or changes in motor planning.
An attempt to find a singular cure all for LBP seems to be a tall order with many factors across physical and psychosocial playing a part.
A Prospective study of back pain of 3,020 aircraft employees “A prospective study of work perceptions and psychosocial factors affecting the report of back injury” (1991) found that job satisfaction was a key factor in developing back pain. Subjects who ‘hardly ever” enjoyed their job were more 2.5 times more likely to report back injury than subjects who ‘almost always’ enjoyed their jobs. The researchers here took into account individual physical, psychosocial and workplace factors. An important point to note is that a history of current or recent back problems was also a factor in future back pain development.
Efficacy
Xue-Qiang Wang et al (2012) carried out “A Meta-Analysis of Core Stability Exercise versus General Exercise for Chronic Low Back Pain” The aim being to study the specific efficacy of a core stability approach. A Meta analysis provides more precision than a single study and also allows for variation in approaches and sample sizes of individual studies however, sufficient homogeneity is required. With many variations between approaches in the catchall term of “core stability” this study type is important.
The researchers here only included RCT’s (randomised control trials) that compared Core stability versus General exercise. They focused on pain intensity, back specific functional status, quality of life and work absenteeism. Out of 28 studies only 5 filled the research criteria. An RCT is regarded as the gold standard approach for determining the efficacy and effectiveness of an intervention in the hope of determining cause-effect relationship between treatment and outcome. Many studies into core stability fail to include all the necessary criteria, such as a control group, that allows us to make worthwhile associations of the intervention, taking out a third factor that maybe linked to intervention and outcome such as natural healing or regression to the mean which can be seen in cyclic pathologies such as CLBP. Hence the small number of included studies in this meta analysis. Sometimes we get a control group that also does nothing so essentially we are studying something against nothing which often favours the something group rather than comparing two differing interventions. However this decision is usually based on ethics. If evidence suggests usual care has no effect, then ethically a ‘nothing’ control group can be used. If however, evidence suggests whether usual care has an effect and the aim is to compare an intervention e.g. core stability exercises versus usual care, then usual care ethically should be given.
This threw up some interesting results. In the short term measures of pain and disability for the core stability intervention were better than for general exercise. However taking into account that we are discussing chronic back pain, no significant differences were observed at 6 months. So although providing some short-term effects, a core stability approach was an ineffective treatment of chronic lower back pain.
Their actual conclusion being
“Compared to general exercise, core stability exercise is more effective in decreasing pain and may improve physical function in patients with chronic LBP in the short term. However, no significant long-term differences in pain severity were observed between patients who engaged in core stability exercise versus those who engaged in general exercise”
One possible explanation for better short-term outcomes for the core stability group could relate to the lower load/intensity of some core stability exercises and therefore a better toleration from the patient. This however is pure hypothesis!
Mannion et al (2012) in “Spine stabilisation exercises in the treatment of chronic low back pain: a good clinical outcome is not associated with improved abdominal muscle function” looked at the link between increased ability to activate the transversus abdominis, obliquus internus and obliquus externus during "abdominal-hollowing" during rapid arm movement. Again this was consistent with the original research parameters from Hodges.
Although some improvements were made in disability and average pain levels pre to post therapy they did not significantly correlate to changes in muscle activation. Of the muscles tested only the TvA made any improvements in voluntary contraction, this being 4.5% (P=0.045).
They conclude that
“Neither baseline lateral abdominal muscle function nor its improvement after a programme of stabilisation exercises was a statistical predictor of a good clinical outcome. It is hence difficult to attribute the therapeutic result to any specific effects of the exercises on these trunk muscles”
Marshall et al (2013) looked at “Pilates exercise or stationary cycling for chronic nonspecific low back pain: does it matter? a randomized controlled trial with 6-month follow-up”
Again we see in this study that in the short term targeted specific lower back (SEG) exercises seem to have a better outcome than less targeted interventions. In this case cycling. Disability was significantly reduced in specific trunk exercise group after 8 weeks as was pain but to a lesser degree. Fear avoidance beliefs were reduced in the SEG group after 8 weeks compared to 6 months with stationary cycling group.
At 6 months however no difference between the two groups was reported with regards to clinically meaningful changes. As the patient group was of the chronic nature short term measures of success are less important than longer-term outcomes. In the longer term as the results for both interventions are similar the authors conclude that we could recommend either for chronic LBP.
Are the short-term outcomes for core stability interventions attributable solely to core stability or another mechanism such as patient beliefs? It would be useful to understand why the improvements are better in the short term versus the lack of long-term efficacy when compared against more general interventions.
Interestingly the researchers had this to say:
“The magnitude of improvement in self-report measures reported in the SEG may have been confounded by a number of participant biases toward receiving Pilates, a clinically more common type of exercise rehabilitation for LBP compared with stationary cycling”
Core stability is well marketed for cLBP whereas patients may perceive general movement to be damaging even though the long term outcomes are similar.
Conclusion
Although we see some short term benefits with ‘core stability’ exercises compared to more general exercises this approach does not seem to be more effective over longer time frames. Considering the needs of the patient group are of a chronic nature this type of intervention would have to be regarded as ineffective as a specific form of treatment in chronic patients. Could receiving a perceived clinically ‘relevant’ treatment influence short-term beliefs? Or perhaps better tolerated due to lower loads? It would be interesting to shed more light on the possible mechanisms behind this.
The proposal of a stereotypical adaptation to pain and, therefore intervention may not be a true reflection of the many and varied muscle activation adaptations to pain that are available to the CNS. The muscular activation pattern of the cLBP patient is likely to be individual and task dependent based on more modern EMG research findings into adaptations to pain (Hodges 2011).
Timing of muscle activation does not seem to positively or negatively correlate with reduction in pain levels or perceived readiness for return to work. Attempts to change timing of activation would appear to make little impact on actual onset of activation.
Approaches that combine a view of pathophysiological, motor control and psychosocial factors may stand the best chances of success, although a review of these approaches is the not the aim of this piece.
Many movement and motor control exercises maybe beneficial for cLBP. It is possible that no one form of intervention is right for all cases, especially in light of variable activation strategies and this seems to be highlighted by the research findings.
An increase in variation in available movements and specific movement strategies based around the individuals functional deficits and task specific needs may yield the best results with a movement based problem.Treating the individual would appear to be the only option if we can find no objective deficit to treat.
A generalised approach to exercise may be no better than an approach using ‘core stability’ exercises generically when a focus on individuality is used. As with most chronic injuries education about pain, movement and relationship to pathology alongside other applicable interventions maybe the best course of action.






Comments are closed.