Functional ACL strategies – Part 2 (of 3)
In the second part of this 'Functional ACL strategies' blog, which has now become a three parter, we consider some more of the issues surrounding ACL rehabilitation and prevention.
The main focus of this blog is on neuromuscular skill and associated processes with relation to the specific movements associated with ACL injury we explored in part one.
In Part 3 we will show some exercise strategies and progressions for ACL injuries.
You can read part one by *Clicking Here*
Training to avoid the movement or training the specific skill?
It seems there maybe two distinct camps when looking at movement associated with injury and the rehab & prevention process.
One would be to attempt to avoid the motions altogether by 'strengthening' the associated musculature. In the case of the ACL often the lateral hip to create an abduction moment to counter act the adduction of the femur and relative abduction or valgus of the knee joint that is associated with the injury.
Another view is the shift towards neuromuscular skill training. This move away from just strengthening has seen success in ACL prevention and gait retraining for a number of different injuries. This methodology looks at retraining the specific skill itself rather then the muscular components that would work in unison in task specific patterns of activation. The specific kinematics and movements were highlighted in the first part of this blog series.
It could be teaching the motor system the specific neuromuscular skill to control/decelerate the motion of femoral adduction maybe more beneficial than strengthening the abductors to resist the motion through non-specific movements.
Reducing dynamic valgus at the knee has also been implicated in Patella femoral pain as well as ACL injury and has some relevant research that can be looked at.
Ferber (2011) found no reduction in peak knee genu valgum angle even though increases in hip abductor strength and decreased pain were reported after a 3 week hip-strengthening program. Interestingly the increased strength did not change the kinematics, which would be associated with an ACL injury, although it did have an affect on pain levels and decreased variability of motion at the knee joint.
Kleim (2008) lays out some specific elements of experience dependent neuroplasticity that would be required for the neuromuscular skill acquisition associated with ACL rehab & prevention.
They include:
• Use It and Improve It - Training that drives a specific brain function can lead to an enhancement of that function.
• Specificity - The nature of the training experience dictates the nature of the plasticity.
• Repetition Matters - Induction of plasticity requires sufficient repetition.
Willey and Davis (2011) also found that specificity of training was important. They used a single leg squat program, including strengthening and neuromuscular retraining elements, that increased strength in hip abductors and reduced hip adduction in a single leg squat but not during running. The conclusion was that non specific strengthening and movement training did not alter abnormal running mechanics. This shows changes are likely task specific in relation to neuromuscular training.
We can choose to retrain the neuromuscular mechanisms in the key movements associated with ACL injury to reduce the amount of movement the knee goes through and success has been had with combining a number of feedback tools to aid this process.
Neuromuscular training has been performed with some success by Hewitt (1996) to reduce valgus torques at the knee focusing on the neuromuscular control of landing. Although the landing was on two legs rather then the one generally seen in ACL injury.
Hewitt’s prospective (1999) study of neuromuscular trainings effect on injury rate showed significant effects on the injury rates between the untrained female athletes vs the trained group. The untrained group having a 3.6 times higher incidence of ACL injury versus the trained group. Both injuries in trained group being contact in nature.
The training for the Hewitt study was focused on the vertical jump. A function specific approach could focus on the components associated with the mechanisms of injury, as laid out in part one, to produce the most specific neuromuscular learning experience in a controlled environment. These components would include a single leg, multi plane kinematics and increased speeds and ranges. Proprioceptive training has been shown to significantly decrease incidence of ACL injury (Caraffa 1996). This could be improved through specific and authentic stimulation of the proprioceptive system in relation to mechanisms of injury and demands of sporting movements.
Strength & skill
Strength is a major component of sports performance. Often we look at isokinetic tests of strength in individual muscles. This can throw up some useful data. Abrams et al (2014) in a systematic review of functional testing after ACL reconstruction found Knee extension strength lagging behind knee flexion strength with all graft types with isokinetic testing.
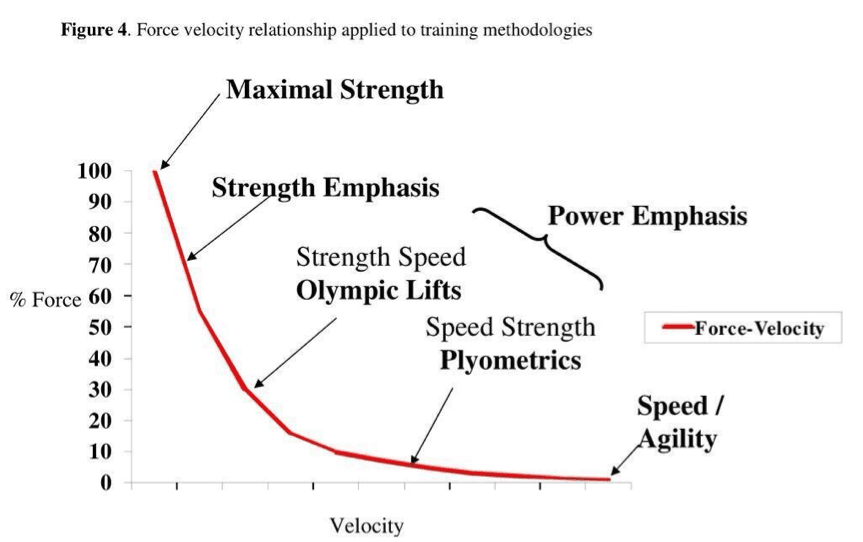
The key question is do isokinetic measures of strength give us a good indication of return to play readiness? Isokinetic contractions rarely happen outside of the laboratory. There are achieved by velocity remaining constant while force is allowed to vary with the use of expensive machinery. This is the opposite of how force is created in a functional environment such as sport where we often against a low mass we have to increase velocity to create force. Angelozzi (2012) found significant deficits in the rate of force development after ACL reconstruction even though maximal voluntary contractions had almost returned to pre injury levels. Both in terms of testing and rehabilitation the neuromuscular skill of rate of force development must be taken into account. A major contributory mechanism of ACL failure seems to be high speed.
How does this influence our practice? Strength is often determined by mass during training and rehab. Strength is force applied to an external object with a bias on the mass part of the F = MA equation. Rate of force development against lighter loads or even in fact no external load is also important. Force has to be created and controlled across a huge variation of vectors. Force is vectorial meaning it possess both a directional and magnitude component. Landing, associated with ACL injury, is more about the control of force acting on the body through deceleration rather than active creation of force.
Force is also summated and dissipated through the coordination of multiple passive and active segments moving through changing relationships in a complex multi dimensional functional movement. The neuromuscular skill of coordination of the leg as a whole maybe primary to the individual testing or strengthening of muscles.
Strength is often specific to a movement or skill. In fact we see very little crossover between the skills of different lifts such as the squat and deadlift (Hales 2009) that are often used as strength exercises during rehab. It could be argued that these are much more similar movements than a landing or cutting maneuver, through being bilateral and fairly uni-dimensional in comparison, and are often dominated by mass. Traditional resistance exercises focusing on strength and power variables display only a small to moderate correlation with change of direction performance which is a key component of cutting motions associated with ACL injury (Brughelli 2008)
This begs the question of crossover to return to play and the concept of generic strength exercises for a specific movement although physiological changes such as tissue tolerance maybe impacted.
Cortical representations and task specific neuroplasticity.
If we have more focus on neuromuscular skill then we also must consider the brain areas associated with movement skill such as the cortical representations of our physiology in the primary sensory and motor cortex. Pain has consistently shown to have an effect on the motor system (Tsao et al 2011) and muscular activation and inhibition. Although these changes are often individual and non stereotypical. (Hodges & Tucker 2011)
Changes to the cortical representations have been hypothesized to be vital to long term rehabilitation success (Falla 2010) This makes sense when we appreciate the changes pain can have on the sensory and motor areas. Altered motor performance maybe a factor in the maintenance of pain (Falla 2010)

Experience dependent plasticity is related to changes in the brain in response to a specific stimulus or experience (Doyon 2005) With relation to ACL injury this could be negative changes associated with reduced movement during pain or immobility. Positive changes would be associated with rehabilitation especially if functional needs of the physiology/neurology are taken into consideration.
Strength training does not achieve the same affects as skill training in the brain. The ability to target specific movement components, such as required for the motions associated with ACL injury, requires increased levels of attention and precision than the co-contraction of muscles (Falla 2010)
Movement behaviour has been reported to be independent of strength. This may suggest post training changes in movement are a result of improvements in motor skill. (Mizner 2008)
Novel motor skill training, in contrast to passive treatment or more generalized exercise, has been associated in improvements of task performance, cortical excitability and increased cortical representations (Sedato 2001, Pascual-Leone 1995, Karni 1995).
Skill training combined with strength training created no more changes to the primary motor cortex than skill training alone (Remple 2001) this is highlighted by the inability of strengthening of the lateral hip muscles to reducing knee valgus as discussed earlier and neuromuscular training being successful for reducing ACL occurrence & re-occurrence.
Lasting changes after skill acquisition have been shown to be retained 6 months post training with ACL prevention training (Powers 2010). This has been shown via diminished corticomotor excitability suggesting sub cortical structures such as the cerebellum now being more involved in the motor output. This may suggest a more subconscious ingrained strategy associated with ‘neural grooving’ (Beck 2007, Powers 2010)
Movements when fatigued
Fatigue is implicated in higher incidences of injury such as fixture list congestion (Bengtsson H 2013). Fatigue has an effect not only on the ability to create force but also on smooth and controlled movement (Cortes et al 2013). They performed a very ACL injury relevant piece of research using side stepping cutting task. They found an increase in variability for knee kinematics and moments following exercise-induced fatigue. Ferber (2011) has also implicated variability of movement at the knee in patella femoral pain. As variability increases due to fatigue we may see a decrease in neuromuscular control associated with reduced knee valgus.
Movement assessment when fatigued may give us a clearer picture of capabilities of an athlete and their risk of injury or re-injury. The task specific nature of neuromuscular skill acquisition may also benefit from training with the focus on the specific concurrent variables of fatigue and movement control.
With this in mind movement training specific to ACL injury prevention could be cycled to different times within a training schedule including both pre and post training and stand-alone sessions.
It would also be beneficial during a rehab program to vary levels of fatigue as an assessment variable and also an additional controllable variable for adaptation
Graded Exposure
Pain changes motor behaviour and movement responses. A driver of this motor behaviour may be to protect from further pain or damage to a tissue. This may also include perceived damage. Hodges & Tucker (2011) proposed some key characteristics of motor adaptations after pain.
Their theory sees modified movement and stiffness at multiple levels of the motor system (such as supraspinal) that are often implemented in a non-uniform manner. The motor and muscular strategies are often highly individual and inter and intra muscular activity are not stereotypical as some have previously proposed. These motor adaptations may have short-term benefits such as an ongoing protective motor behavior to avoid further tissue damage but potential long-term consequences after the tissue healing process has completed and previous movement ability remains altered.
This maybe apparent in non-copers after ACL injury who display different gait and muscular contraction patterns to copers. Higher levels of co-contraction, distinct gait adaptations can be present along side reduced knee motion and moments (Rudolph 2001)
We also see Kinesophobia, a fear of movement, is associated with knee function after ACL surgery (Hartigan 2013). This also might be part of a sub conscious protective strategy.
With fear and protective strategies present the more we ask of the neuromuscular system to cope with, the more we may get a protective response that perhaps does not correlate with the level of danger perceived by the brain. With this in mind a successful strategy would introduce a graded approach to restore the ability of the motor and sensory systems to deal with a full spectrum of functional variables including ROM, speed and instability challenges.
Interestingly Swaink et al (1999) found that the absence of side-to-side differences in muscular adaptations, hypothesized to give functional stability in ACL deficient females, suggests that these adaptations occur bilaterally after ACL injury. As most functional activities involve concurrent movement of multiple limbs this could show a body wide protective strategy that fits with Hodges and Tuckers theory of system wide intra and inter muscular changes.
Protective motor adaptations could be assessed by increasing the demand level of a specific movement and the associated variables. Observing the motor systems change in movement and stiffness levels may indicate an increase in protective response and guide the appropriate level of demand for the current state of the CNS.
We must also think about the role the ACL itself plays in the neuromuscular process. A wide range of afferents that contribute to proprioception and reflex activation exist in ligaments. The compromises after injury are not just mechanical but also kinesthetic and reflective loss associated with enforced joint stability that maybe implemented as a protective response to previously harmful experience (Solomonow 2003).
Reflex activation of muscles by stimulation of the ACL is thought to prevent distraction of the joint and reduce strain on the ACL (Solomonow 2003). There may also be inhibitory effects of the ligamento-muscular reflex to reduce large forces from developing in the muscles that would increase stress on the ligament. So the ligamento-muscular reflex maybe either inhibitory or excitatory in the pursuit of creating joint stability and reducing strain on the ligament.
Neuromuscular training would be designed to recalibrate these elements of the neuromuscular process through a graded exposure to function related movements. This would provide not only physiological/mechanical properties but also a range of multi plane tensions and compressions for afferent feedback to the spinal reflex mechanisms and supraspinal components of the neuromuscular system and a congruous relationship between perceived and actual level of threat to the ACL. Timing and level of muscular activation would be relative to the demands of the task and involve a task specific learning experience including the appropriate motor responses.
References
- Tsao H, Danneels LA, Hodges PW. ISSLS prize winner: Smudging the motor brain in young adults with recurrent low back pain. Spine (Phila Pa 1976). 2011 Oct 1;36(21):1721-7. doi: 10.1097/BRS.0b013e31821c4267.
- Remple MS, Bruneau RM, VandenBerg PM, Goertzen C, Kleim JA. Sensitivity of cortical movement representations to motor experience: evidence that skilllearning but not strength training induces cortical reorganization. Behavioural Brain Research 2001;123(2):133e41.
- Karni A, Meyer G, Jezzard P, Adams MM, Turner R, Ungerleider LG. Functional MRI evidence for adult motor cortex plasticity during motor skill learning. Nature1995
- Doyon J, Benali H. Reorganization and plasticity in the adult brainduring learning of motor skills. Curr Opin Neurobiol. 2005;15(2):161–167.
- Mizner RL, Kawaguchi JK, Chmielewski TL. Muscle strength in the lower extremity does not predict postinstruction improvements in the landing patterns of female athletes. J Orthop Sports Phys Ther., 2008;38(6):353–361.
- Hales, Johnson and Johnson, Kinematic analysis of the powerlifting style squat and the conventional deadlift during competition: is there a cross-over effect between lifts? Journal of Strength and Conditioning Research, 2009
- Beck S, Taube W, Gruber M, Amtage F, Gollhofer A, Schubert M. Task-specific changes in motor evoked potentials of lower muscles after different training interventions. Brain Res. 2007;1179:51–60.
- Ferber R, Kendall KD, Farr L. Changes in Knee Biomechanics After a Hip-Abductor Strengthening Protocol for Runners With Patellofemoral Pain Syndrome. Journal of Athletic Training 2011;46(2):142-49 -
- Boden BP, Dean GS, Feagin JA Jr, et al. Mechanisms of anterior cruciate ligament injury. Orthopedics. 2000;23:573-578.27.
- Hewett TE, The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med. 1999 Nov-Dec;27(6):699-706
- Caraffa A, Cerulli G, Projetti M, et al: Prevention of anterior cruciate ligament injuries in soccer. A prospective controlled study of proprioceptive training. Knee Surg Sports Traumatol Arthrosc 4(1): 19 –21, 1996
- Rudolph KS, Dynamic stability in the anterior cruciate ligament deficient knee. Knee Surg Sports Traumatol Arthrosc. 2001;9(2):62-71.
- Hartigan EH et al, Kinesiophobia after anterior cruciate ligament rupture and reconstruction: noncopers versus potential copers. J Orthop Sports Phys Ther. 2013 Nov;43(11):821-32.
- Paul W. Hodges ⇑, Kylie Tucker, Moving differently in pain: A new theory to explain the adaptation to pain, Pain, 152 (2011) S90–S98
- C. Buz Swanik, PhD et al, Reactive Muscle Firing of Anterior Cruciate Ligament-Injured Females During Functional Activities, J Athl Train. 1999 Apr-Jun; 34(2): 121–129.
- Brughelli M et al Understanding change of direction ability in sport: a review of resistance training studies. Sports Med. 2008;38(12):1045-63.
- Solomonow, Ligaments: a source of work-related musculoskeletal disorders, Journal of Electromyography and Kinesiology 14 (2004) 49–60
- Kleim J, Principles of experience-dependant neural plasticity, Journal of speech, language and hearing research, Vol 51. Feb 2008






