Pain education – What might make it MORE effective?
Pain education is a valuable tool for some, but certainly not all, patients. It can help to provide a narrative or explanation for problems that may remain unexplained by ‘traditional’ medicine or therapy.
This paper HERE regarding chronic lower back pain explores what people are looking for from a visit to a therapist.
“more than 90% of patients expected a physical examination, tests or investigations, a diagnosis, reassurance and advice, and clear explanations of causation, symptom management”
How tough is this in many instances with no clear diagnosis or causation available?
Up to 90% of back pain is described as ‘non specific’ for this very reason. We know that uncertainty is a big deal for many patients. Mishel first proposed this in the “theory of uncertainty of illness” HERE.
Carroll's paper HERE “How Well Do You Expect to Recover, and What Does Recovery Mean, Anyway? Qualitative Study of Expectations After a Musculoskeletal Injury” also discusses the process of diagnosis, uncertainty and the subsequent effect on expectations of recovery.
But although data suggests pain education can help it can also be very tough to deliver.
This quote from Louis Gifford sums it up nicely.
"The patient that learned from their pain explaining therapist that their pain didn't really mean anything, who suddenly got out of the chair, went home and went riding their bike for the first time in 5 years...just doesn't really exist!”
So how can we improve the delivery of pain education?
A question I often ponder is have we replaced anatomy with neurobiology? Do we now bombard people with complex processes involving brains, nerves and receptors rather than complex biomechanical stories? How much neurobiology or neuroscience is actually required?
In some cases certainly it will be useful, but in many cases maybe it could actually hinder. This does not mean that some of the key concepts such as plasticity, sensitization and the brains role in pain are not important but maybe the minutia of information that can be focused on is unnecessary.
Perhaps we can apply some of the information in this paper HERE. Simplifying MRI reports appears to have a positive effect on how they are received. This may also apply to the delivery of pain education. What does nociception or Ion channel mean to a patient? It could end up very similar to VOMIT (Victims of Medical Imaging Technology) HERE if poorly delivered.
Should the focus now be on the delivery and context of information rather than the information itself?
Contributions
I thought it might be nice to get some other opinions on some of the key elements that go into making successful pain education and reached out to colleagues from around the world, using social media, to pitch in.
Some of the key components I already advocate, but I must admit some others I had not considered and provide valuable food for thought for myself and perhaps also the wider therapeutic community.
I was pleasantly surprised by the elements discussed, almost none related to the actual information itself but instead on the delivery and thought process involved.
Here they are!

Listening
The most consistent point made by the contributors as a whole was listening.
Listening is a key clinical tool. Although pain education is often thought of as the delivery of information, it should start with listening. I think this is advocated on many fronts but as we know patients can often be interrupted pretty quickly HERE and this is always worth keeping in mind.
The desire to be listened to also appears to be valued from a patient perspective and helps to build therapeutic alliance HERE. This is probably vital for those receiving and processing the information. delivered.
This is a good paper on ‘listening as therapy’ HERE
Validation
A couple of patients also contributed to the discussion and they felt that someone listening to and validating their experiences was a big part of their recovery. This also ties into the paper above regarding a patient’s perspective. If symptoms cannot be ‘medically’ explained or solved by traditional interventions, then patients may feel that they are being seen to ‘make it up’ or exaggerate their painful experience. All pain is real and although it can often be hard to describe it is also exactly the way that someone says it is. It cannot be anything else!
Individualisation
Another of the key points consistently put forward was about individualizing the delivery and placing into a relevant context. Now I personally have a bias for placing pain education in context with someone’s current situation. By weaving it into their story and using their painful examples to tie in some of the key concepts I think we are more likely to get some elements of comprehension.
This fits well with the key component of listening. Without listening we cannot place the information in the context of the patients narrative.
The question is, is this more effective than information generically delivered? I just don’t know. I think this would be an interesting comparison to study.
Asking!
One thing I must admit to NOT asking was simply “do you want to know more about pain?” This was brought up by a number of people. This may avoid the very real problem of ramming pain science where it is not wanted. Pain science should be judiciously applied where it is needed AND wanted rather than a therapist dropping knowledge bombs expecting an instant epiphany.
It is not a passive exchange
Remember there are two equal people involved in this. It is not simply a teacher pupil relationship. Patients lived experiences are also important. The therapist can also learn from the patient, especially when it comes to the patient experiences. Perhaps it should be seen as a journey by two people to find mutual meaning in a negative situation rather than simply an educational experience.
Pain science is a way of thinking not an intervention
One of the criticisms that I have seen recently of the application of pain education is that it is seen as a standalone intervention. So rather than bombarding people with statements or analogies that have been previously heard for explaining pain, the concepts and ideas should affect the way we reason, interact, explain and apply the treatment provided.
Experiences are as powerful as talking
It’s not just about talking; doing is also a powerful educator. Perhaps sometimes talking is needed before and after the doing, but without the actual doing we cannot ‘prove’ the point. Beliefs about the body are a good example of this. Without SEEING or FEELING a different, positive outcome to that expected, potentially a number of times, a belief may remain in place.
Again listening is key. What are the key experiences that need to be reconceptualised in a physical sense as well as a cognitive sense.
Find out HOW your education has been interpreted
As with any part of the therapy process, pain education has the potential to have a NEGATIVE outcome as well as a positive one. We may well baffle people with talk of brains and outputs etc and HOW they interpret this information is the arbiter of success, however well meaning or comprehensive the input by the therapist.
This may boil down to wording, health literacy and therapeutic alliance. The list of potential influencers is endless, but essentially the ability to mitigate any negative effects could be dependent on simply asking!
We may be able to influence this interpretation by being clear and concise, using bite sized chunks of information, avoiding confrontation regarding beliefs and also avoiding negative or long winded medical or anatomical jargon and terms.
Reflective questioning
Don't just providing statements, also use reflective questioning. This may help to facilitate understanding and apply this new information to their own personal experiences and think critically about some of the beliefs they may hold.
Lets say someone has a negative belief regarding about their back because of a slipped disk a number of years ago. We could suggest that structure and symptoms don’t always display a consistent relationship. We could follow this up by asking if their symptoms come and go (as long term back pain generally does) and would this be a sole cause if the ‘slipped’ disc remained a constant.
Of course this is just some opinion/s but collectively they could be valuable!
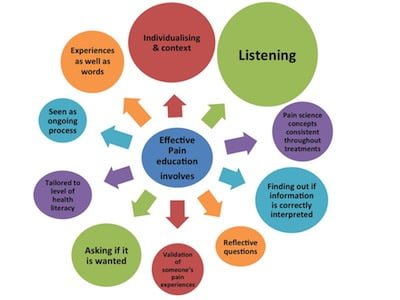
Key points
- People are looking for answers
- Uncertainty makes things worse
- Pain education may provide some explanation
- It is tough and often fails
Some things may make it more effective
- Listening
- Validation
- Individualisation
- Asking If it is wanted/needed
- It is not a passive exchange
- Pain science is a way of thinking not an intervention
- Experience is as powerful as talking.
- Find out HOW your education has been interpreted
- Reflective questioning








{kind=link}
{kind=link}
Leave a Reply
Want to join the discussion?Feel free to contribute!