WTF does functional mean anyway?
Functional is a word banded around in training, rehab and therapy regularly but what does it really mean? Is there a definition?
It maybe that it means different things to different people or in fact means nothing at all! Some terms we use here are "movements that matter" or "meaningful movement" for this very reason but like all buzz words people seem to like and identify with "functional" or sometimes have very strong negative feelings about the term.
Functional, either assessment or treatment, could simply mean that it is not clinical, less passive and more active movement. It is important to have more than one perspective. It is becoming more obvious that what happens in one context is not simply reflected in another. As most people spend their time out of a clinical environment in the course of their lives this is a valuable perspective in my opinion.
It could also mean a move away from not just seeing the body as isolated muscles and joints and basing exercises around this principle but also relevant movements with interacting parts.
Can we refine these general principles a little further to enhance our results? An appreciation of the specifics matters too. If we want to improve our running skill or change the skill to modify pain then we have to understand more about the function of running and how the client runs, hence the emergence of gait retraining.
My first thought about functionality is wanting to be client centered. This means that rather than picking a set of movements I have been told are ‘functional’ by some ‘guru’, a course I have been on or seen on a YouTube video I am thinking about what is functional for the individual standing in front of me.
Can we objectively define what is functional for the individual standing in front of us? I struggle with this idea.
The individual
Imagine an elite soccer player or a grandma. Both are going to have different needs, wants and tolerances. They may have differing specific movements that they would like to perform, either pain free or with an increase in performance. Sure a squat pattern will be a great functional movement for both of them, but the exact same squat? The different ways we could potentially squat are enormous.

The Grandma may want to squat with a forward bend with various rotations to prune her roses more comfortably. The soccer player may need to squat with a variety of leg widths to accommodate the demands of the game. The Grandma may want to be able to stay in that position for a duration of time, the soccer player to get in and out of position as quick as possible.
Both may need capacity, variety and variability in their repertoire of available squat patterns for environmental factors such as differing terrain or reacting to the opposition/reaching for the ball or in the case of the Grandma reacting to a slip. For both a traditional gym squat may not cover all the bases for their needs. It does not mean we can't use a traditional loaded squat but can we adapt also it and make it more applicable.
This increase in capacity, variety and variability could be the difference between re-injury or pain free function. This is certainly functional in my opinion.
In this way it becomes very hard to define what functional is. Instead I see functional as:
“An appreciation of the needs of the individual and helping them to carry out or improve those needs”
It is really hard to break functionality down into a number of assessments, screens, movements or definitions. The rigid protocol may have to be replaced by a variable reasoning process. That seems to be true in many areas of training and therapy.
Input and output
There seems to be two schools of thought here when discussing the word ‘functional’.
One would be that input has to look like the function to get a desired output. That may mean that to improve the golf swing we would need to perform more exercises looking like a golf swing. The other that the input can be anything that gets us a favorable output. So we could do something not directly related in terms of replication of a movement but gets rid of pain or improves the length of my drive for example.
I subscribe to both theories.
Increasing our movement capacity around a joint may allow us to perform many functions better. It may not look like any single function but impact on the performance of many. Equally helping the nervous system deal with different positions and stiffness levels could desensitise the protective motor system responses we may see after an injury. Again this may be non-specific but affect many specifics or level of pain.
It may also be that if you want to improve a specific movement, one that causes pain or perhaps is important to performance, like a serve in tennis for example, we may also have to appreciate the specific movement itself. Imagine if I were getting a neuropathic pain only at a specific intensity during a specific movement then I would want someone to appreciate the skill (motor/sensory pattern), biomechanics and neurodynamics involved. How often do people say “I get pain when I do XXX”? If so then we need to evaluate that context.
Strength training will have general physiological effects on the body that can improve many different functions. Equally we may need to train specific movements and force vectors to ensure crossover to improved performance in a desired sport.
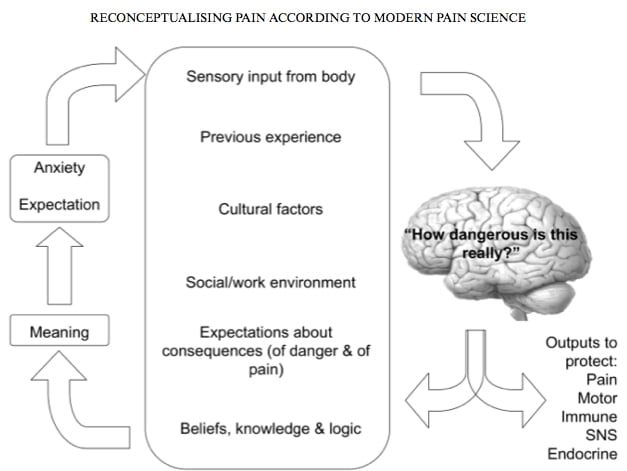
We may find after an injury the perceived threat level of a movement to the CNS increases. That makes sense. Once bitten twice shy. Pain is one of our alarm systems. We can choose a number of outputs such as pain & motor system responses in the face of danger in order to protect. We know that the response of the protective mechanisms do not always correlate with actual level of threat.

One area of functionality that often needs to be restored is the calibration between the actual level of threat of a movement and the way the nervous system perceives it. There are many factors the body uses to determine danger level. These include sensory feedback and previous experience. Simply put this means that putting the body back in a context that has previously caused it harm may elicit a changed response to the context. So we may have to be very specific with movement patterns and variables, such load and speed, to get a harmonious response to the desired action. This often means starting at a tolerable level and grading the exposure to finally reach a functionally authentic level of intensity in a relevant movement. This specific process maybe missing in many rehab programs and could be a factor in re-injury when in a more functional context. This will also be true of tissue and exposing it to the relevant force vectors for structural adaptation.
The SAID principle will always have a place. Swimming may affect my aerobic health that could affect my golf, but I would still want to practice my putting!
Rate of force development is a variable we may see more in a functional context rather than a clinical one. Having to accelerate our mass across a football pitch for example. It is also a variable we often see underdeveloped in ACL reconstruction patients even after more traditional clinical variables such as max strength have been restored.
Getting rid of pain is one thing. Getting rid of pain and being robust enough to be able to returning to unrestricted activity without fear is quite another. If you have not achieved this then you are probably not ‘functional’
It would seem like most of what we do it is a continuum that involves both ends of the spectrum. I can do things unrelated to function that gets me a functional outcome but equally may have to appreciate function to get a functional outcome. It may however all come back to our reasoning process centered around the individual and bridging the gap between where they are right now and where they want to be.
Functional Criteria
So if we want to bridge the gap then we have to know first what is on the other side right? How far, how high etc, otherwise we don’t know how to construct the bridge.
I have some simple criteria I use that I feel reflect the functional demands of our environment. In this way we can also be generally more functional without always being totally specific. People’s movement experiences and abilities are generally eroding as we experience less varied movement habits with our modern lifestyles. What does this mean for the health of our nerves, muscles, connective tissues and brain?
Active
Driven by the client. Creating an active learning experience to change movement skill and pain responses. Perhaps also breaking habits, behaviors and patterns.
Integrated
Movement across multiple segments and using the kinetic chain. This way we can summate and dissipate force across more of the structure.
3 Dimensional
Most ‘exercises’ are limited in terms of exploring our multi dimensional world and articular environment. In this way we can increase our movement capacity and variety.
Moving our COM (centre of mass)
Successfully controlling our COM. Think walking, running, throwing. Most functions involve decelerating and accelerating our COM at some point.
Task driven
Most of our movement is driven by the desire to carry out a task, not to activate individual muscles. Lifting, pulling, reaching and bending are some examples. Each of these activities would need to be carried out in a variety of ways not one specific version.
Interacting with forces
Exposing ourselves to gravity and ground reaction forces that need to be tolerated and harnessed. This may need to be graded.







