Is your anterior pelvic tilt slowly killing you?
Now there’s a sensational title to draw you in! Admit it I got ya!
I thought would do a quick bloggy thing on anterior pelvic tilts (APT) and the associated problems they may cause based on a recent discussion I had. It is certainly not an original post by any means but it is a topic that will not die. In fact any blog post out there that focuses on a bit of the research into this topic rather than just the theory is just a drop in the ocean compared to the mountains of well…stories really. These pieces tend to be thick on biomechanical theory of X pulls Y and causes Z (generally pain) but much thinner on any real science to back it up.
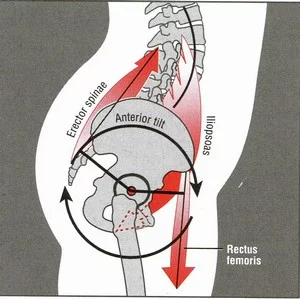
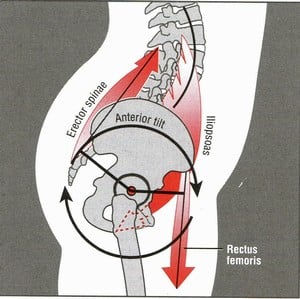
That theory may go a bit like this. You sit too much therefore your hip flexors get tight which pull your pelvis into an anterior pelvic tilt that increases your lumbar lordosis which gives you your back pain.
The humble APT is blamed for all sorts from lower back pain to groin pain and hip pain, in fact any pain that is remotely connected to anywhere close to your pelvis, which being the mid point of your body could be a whole bunch of things.
Go on ‘doctor google’ or facebook (and any social media) and there is steaming piles of this shit in abundance – This is page one of typing “anterior pelvic tilt” into google.
Firstly it is important here to have a bit more knowledge of what is normal and not normal when it comes to pelvic tilts. With so much blame held against the poor ol' APT surely it must be linked, or the associated factors such as increased lordosis, in the available research to all these problems and much more prevelant in painful than asymptomatic populations.
This study "Assessment of the degree of pelvic tilt within a normal asymptomatic population" wanted to find out that exactly that. They looked at the pelvic tilts of asymptomatic people, that is those people not in pain.
They found out that most of us have got an APT, in fact a whopping 85% of males had one. That means take 10 guys in the gym and about eight and half of them will have an anterior pelvic tilt. For women this dropped to 75% but still a majority. If pelvic tilts were to blame for all this pain then surely we would nearly all be walking about in agony in and around the pelvis right? Only 9% of men had the fabled ‘neutral’ pelvic position so if we take those 10 guys in the gym again only 90% of one guy had a neutral pelvis! This was a little better for women going up to 18%.
This is mostly assessed by therapists and trainers in a more rudimentary fashion than the study above, often by identifying bony landmarks, namely the ASIS and PSIS, and their relationship with each other.
This study "Variation in Pelvic Morphology May Prevent the Identification of Anterior Pelvic Tilt" found some pretty large variations in both front to back and side to side bony symmetry. It may seem that the pelvis is all out of whack but in reality it may just be your natural bony shape. So palpation may not be a hugely reliable way to measure an APT it seems and in all likelihood in this case the variation is not a problem in the first place anyways.
It is our assumption of needing perfectly symmetrical anatomy and posture to be pain free and it being the normal default we are born with that is perhaps wrong here not the postures we display it would seem.
This idea of neutral or aligned when it comes to posture has spawned 100’s of CPD courses all aimed at restoring or balancing you to neutral. All the evidence points to the fact not many of us are and when it comes to pain it probably don’t matter!
As we discussed earlier an APT is proposed to cause lower back pain by increasing our lumbar lordosis. This study here actually found no difference between the lordosis of women with and without back pain! "Lumbar lordosis: study of patients with and without low back pain"
The same was true here "Low back pain and lumbar angles in Turkish coal miners" with the lumbar angles not correlating with pain.
So most of us will have an APT and they do not seem to correlate with the back pain we experience.
Sitting is one of the major blamed ‘causes’ of an APT. This study "Use of intermittent stretch in the prevention of serial sarcomere loss in immobilised muscle" found that even 30 minutes a day of stretch, such as you would get by simply moving, is enough to maintain a joints range of motion. Now even the laziest SOB you know will have to get up and go to work and make a coffee and stand up to cook dinner etc. In all likelihood this will add up to the required 30 minutes.
This study here "Effect of Changes in Pelvic Tilt on Range of Motion to Impingement and Radiographic Parameters of Acetabular Morphologic Characteristics" looked at the relationship between dynamic pelvic tilt and Femoral Acetabular Impingement (FAI). They propose an increased dynamic anterior pelvic may result in earlier occurrence of an FAI.
Firstly this was a retrospective piece using a symptomatic population. A prospective study may add a little more weight to the theoretically based conclusion.
So how relevant is an FAI, possibly related to an ATP, to groin pain? In this study "Radiographic Prevalence of Femoroacetabular Impingement in Collegiate Football Players" 95%, yes you did read that right, of asymptomatic collegiate footballers had an FAI. Chances are if you play sport and have lots of dynamic movement of the pelvis you may have some form of FAI, there is also a high probability that it will not hurt!
We must also be aware that position and motion are two different things. I could have the fabled neutral pelvis posture, that only 9% of men have, that still dynamically tilts a long way and therefore affects the bony nature of my hip. Equally I could have a pelvis with an small static APT that does not move away from its postural position very much at all. So a static measure may very well not correlate with a dynamic one and without some form of dynamic measurement method would simply be an assumption and we all know that assumption is the mother of all f**k up’s!
In a normal clinical or gym environment how would you measure this dynamic tilt without all the time consuming scanning and modeling used in the study predicting an earlier onset of FAI's?
In my humble opinion our postures may become more problematic and relevant when they don’t move. We have to actually assess whether a specific posture can move and change rather than assume from the static position before we proclaim it to be a problem.
Finally there is not a lot of scientific proof, the plural of anecdote is not evidence by the way, out there that an APT can actually be 'corrected'.
Stop stressing about your own or your client/patients APT and go and do something more productive with your time.








Leave a Reply
Want to join the discussion?Feel free to contribute!