The myth of exercise prescriptions – It’s probably more trial and error than we care to admit
Its nice to have the answer to the problem before you start, that’s why the idea of an exercise prescription is so appealing as it takes away all that nasty uncertainty that makes you have to think : )
But I bet one of the first questions many therapists ask their patients on the second visit is “how did those exercises work for you?”. So, on one hand we want the answers but deep down our experience tells us things don’t always work out the way we want them too.
Why then why do we see it as a prescriptive? Are you treating a condition, outcome measure or an actual person with different needs and functions?
For me, rehab is much more of an adaptive situation that is progressively refined rather than a prescriptive one simply set out at the beginning. We add things, subtract things and adapt things in an iterative process as we gauge the response in chosen outcomes. The intensity, frequency and type are all open to being adjusted according to the person, their needs and the desired outcomes.
Being comfortable with that is key to working with active movement-based interventions in my humble opinion.
Assessment is also a process of refinement; you might change your mind on what the problem as new information comes to light and a hypothesis does not pan out the way you expected it to. Most of what we do is informed trial and error anyway, there I said it!
The initial intervention and its parameters are just a start, a trial to see what happens next, an informed guess even, but this is not really something that seems to be talked about very much. The prescription is much more of a suggestion than we often like to admit perhaps, the supremely funny Trevor Noah describes traffic lights as a “suggestion” in South Africa, which always tickles me.
Even exercise for physical adaptations is becoming less prescriptive. We are discovering that physical adaptations can happen from a whole bunch of rep ranges and loads. Effort and intensity seem to be key to physical adaptations, often the parameters that are never measured in rehab research!
Learning process
Both therapists and their patients should view this as a learning process rather than a failing or being reflective of not knowing what to do. The idea that we have the answers prior is often detrimental as this can the knock confidence in the therapist’s ability and create expectations that are different from the reality of rehab. We often have to experiment and make trade off’s between pain and functional gain.
Data
Research data can be used sometimes as a bit of blunt tool, as can clinical experience too of course. It can be assumed that the patients specific condition, the treatment and the effect of the treatment will all be consistent with what is written in a paper. But if we look closer the reporting of data, it has its own in-built estimate of variability so perhaps we can only ever know how it effects our patient AFTER application rather than before.
Our patient and their exact presentation may not be accurately represented in a piece of research. No paper samples the entire population, only a small portion, hence the reason for confidence intervals. This is the challenge of clinical practice, to marry the data with the person.
This is a fantastic paper from Roger Kerry "Expanding our perspectives of research"
“Some individuals use statistics as a drunk man uses lamp-posts — for support rather than for illumination” A. E. Housman
We also need to appreciate that with a modern biopsychosocial understanding we literally don’t have prescriptions for many of the issues we see. I have said before that one the main things I work on is the confidence to use bodies and engage in things again, what’s the prescription for that again?
Also papers often don’t give a clear outline of what they did anyways. Many times they point to another paper or an appendix that is never looked at. When you do look, key variables are often missing such as intensities, rest times etc. So being ‘evidence based’ with rehab is often not quite what people think it is.
Is it controversial to suggest that the research process does not always reflect the clinical one?
It’s a process
Unfortunately, clinical reasoning is just not sexy. It’s much sexier to proclaim a treatment does or does not work, this seems to hit people in the feels. The nuances of clinical practice often get left by the wayside and bias and polarisation rules the land. The tough bit clinically is reconciling research-based information with the persons individual presentation and their experiences/beliefs etc.
This is not a one-time deal though, the reasoning and refining process should go on throughout a period of care, not just a diagnosis then prescription at initial evaluation and a continuation of this repeatedly.
This was a really nice comment made during a conversation on twitter:
“Evidence-based practice doesn't mean throwing available evidences blindly at the patient but rather its a delicate process of discovering best suited strategies for every individual patients you see” - Nihar Palan
In my opinion the great therapist is not the one with the best prescription or plan, but instead the one that knows what to do when it does not go to plan. Someone who can adapt and adjust accordingly to the changing situations and people that you deal with.
Another way
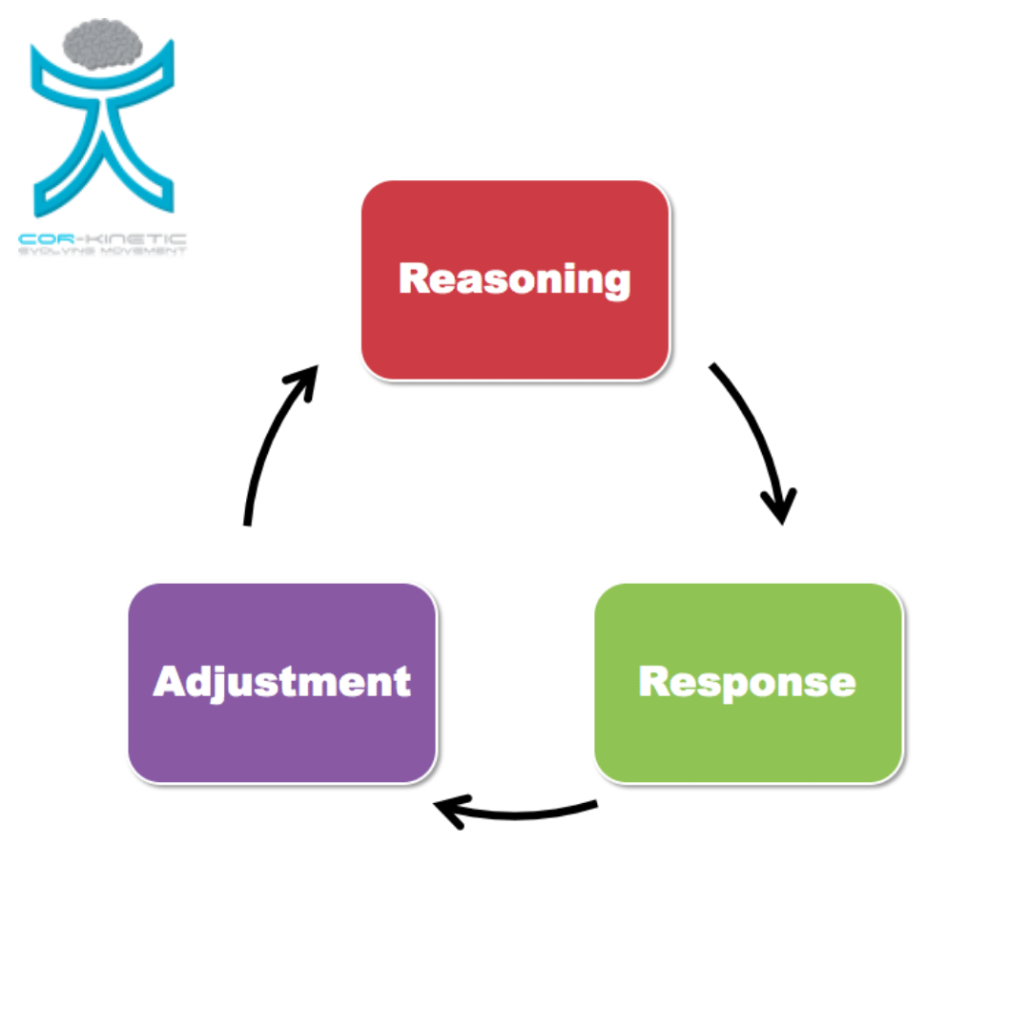
Clinical reasoning
- Research data
- History
- Examination
- Diagnosis
- Application
Response
- What outcome?
- Over which timeframe?
Adaptation
- Stick or twist?
- What to change?
Conclusion
- Prescriptions are really suggestions
- We refine based on response over time
- It’s really informed trial and error
- Research clearly reflects variation in outcomes
- Prescriptions are often not clear in pieces of research
- Knowing how to adapt is a skill, not follow a flow chart
- Reasoning, response & adaptation is a better model IMO
Interested in exercise, movement & clinical reasoning? Come and join us on the 21/22nd November for the "Therapeutic movement & exercise" course *CLICK HERE*








Leave a Reply
Want to join the discussion?Feel free to contribute!